
Health News – February 2022
1 February 2022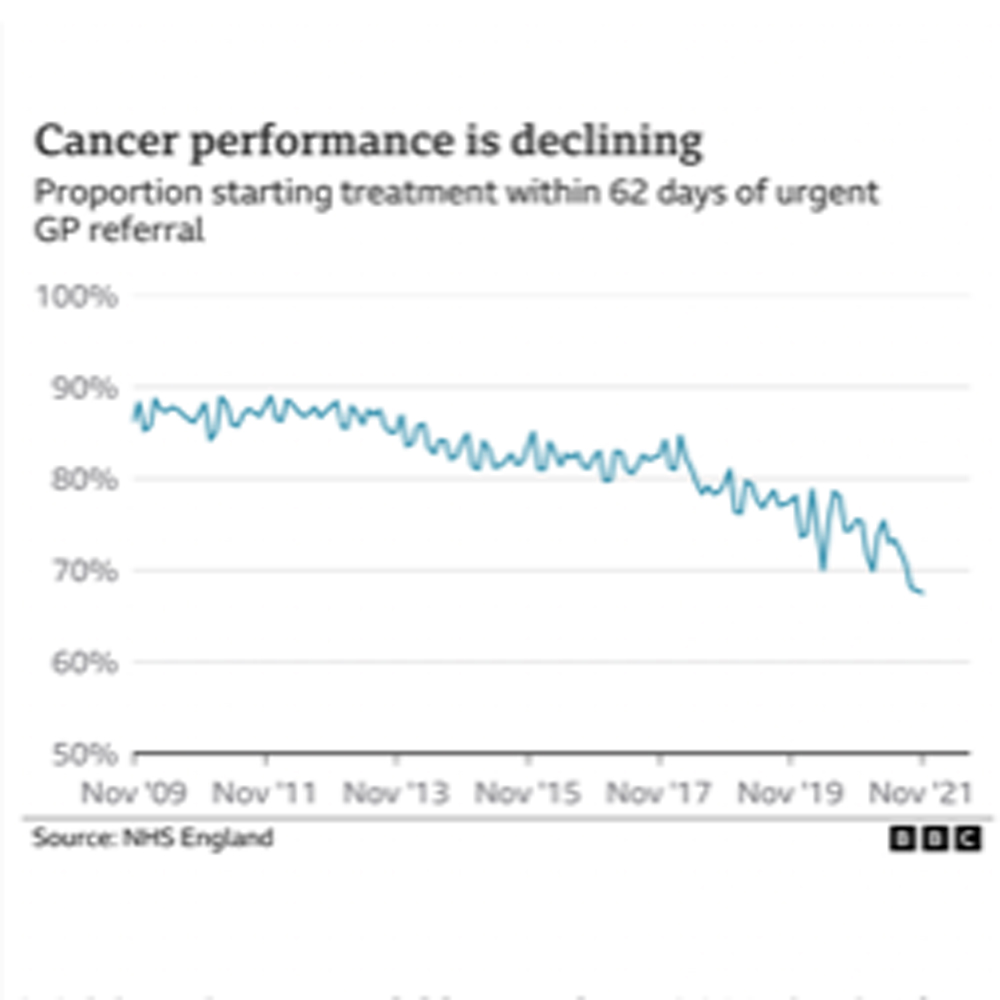
Health News – April 2022
2 April 2022Hello once again dear faithful reader!
Just for you, welcome to another compelling month’s Health News read, to try and take your mind
off of the dreadful atrocities being carried out every day in Eastern Europe currently.
4th Feb – BBC website: Improving Cancer Care a Huge Challenge Post-Pandemic
Ministers promise a new 10-year strategy for England. Figures suggest that there have been 34,000 fewer diagnoses which reduces the chances of survival, cancer charities said. Anna Jewell, chair of the ‘Less Survivable Cancers Task-Force’, said there were particular problems with cancers of the lung, liver, brain, oesophagus, pancreas and stomach, which have the lowest survival rates. Just 16% of people diagnosed with these cancers survive for five years. She continues: “The situation is urgent. If we are to truly be successful, we need to go much further on cancer and improve the persistently poor outcomes that patients in this country have long-experienced compared to other countries.”
7th Feb – Metro newspaper: Coronavirus Cases & Linked Deaths Keep Falling
Cases and deaths linked with Covid-19 have fallen compared with a week ago, figures show. There were 54,095 new infections recorded in the latest 24-hour period, down by 22 per cent on the previous Sunday’s 69,007. Britain’s official death toll rose by 75 to 158,318, with the latest increase 18 per cent down on last Sunday’s 91. The percentage of over-12s who have now received at least one vaccine jab now stands at 91.2 per cent.
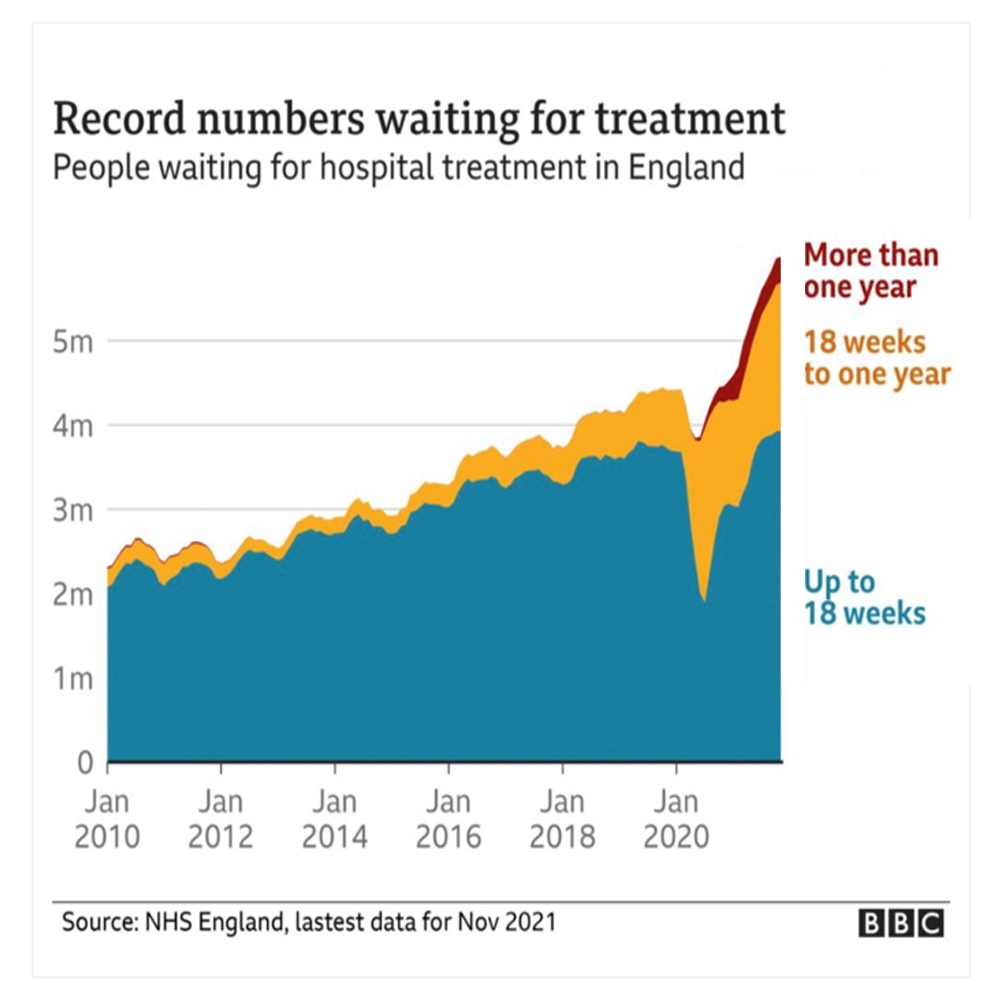
9th Feb – Metro newspaper: NHS Waits May Get Worse Before They’re Better
“The NHS waiting list in England will not to fall for at least another two years – and could double in size”, Sajid Javid has admitted. Outlining the government’s new Covid recovery plan, the health secretary said around 6million patients are queuing for treatment, including hip and knee replacements, cataract surgery and tests. However, he said that, if the 10million people estimated to have stayed away during the pandemic came forward for treatment and activity was not increased above pre-pandemic levels, the waiting list could hit 14million.
11th Feb – Cover magazine: AMII Welcomes Vida Insurance and Surrey Circle Health
The Association of Medical Insurers and Intermediaries (AMII) added Vida Insurance Advisors and Surrey Circle Health as its newest members.
- Based in Bedford, Vida Insurance Advisors was set up by Nick Meek in July 2020 and offers advice on Private Pedical (should’ve read ‘Medical’ of course!) Insurance (PMI), life assurance, critical illness cover, shareholders protection and income protection for both individuals and SMEs.
- With more than two decades of experience in the industry, Daniel Donoghue set up as specialist PMI broker trading as Surrey Circle Health based in Addlestone, Surrey. Donoghue continued: – “I’m absolutely delighted to join the industry’s professional trade association and look forward immensely in trying to help further the ongoing governance of the UKs PMI industry, particularly coming out of the pandemic in both the private and public sectors in this country.”
11th Feb – LinkedIn social media: VitalityHealth Newsletter
- Having looked at 65,000 Vitality members found that both moderate and high levels of physical activity are crucial in improving outcomes, including decreasing the risk of severe illness by up to 45% and death by up to 42%. The moderate levels cited in the study are well below recommended physical activity guidelines, suggesting even some physical activity is beneficial.
- Vitality Health International (VHI) successfully launched a health insurance product across five African countries – Nigeria, Ghana, Kenya, The Democratic Republic of Congo and Zambia. Employees enrolled upon their employer’s company policies will have access to the Vitality ‘programme’ – the world’s leading behaviour change program.
17th Feb – Metro newspaper: Global Cases Fall by 19% in a Week
The world’s death toll is plateauing, according to the World Health Organisation (WHO).
Just over 16 million new coronavirus infections and 75,000 deaths were reported worldwide between February 7 and 13, said the UN Health Agency.
Southeast Asia reported 37 per cent fewer cases, the biggest drop globally.
Meanwhile, Russia saw the biggest number of new infections. Cases there and elsewhere in Eastern Europe have doubled in recent weeks, driven by the surge of the infectious Omicron Variant.
22nd Feb – Metro newspaper: PM – Now It’s Over to You
Boris Johnson has urged people to show personal responsibility as he announced almost two years of Covid restrictions will end on Thursday 24th February. The prime minister said that was the day people in England would no longer be legally required to self-isolate when they catch coronavirus. Routine contact tracing and self-isolation payments will also end under the government’s new ‘Living with Covid’ plan. He warned the pandemic was not over, with the Queen’s positive test a reminder that the virus had not gone away. Continuing Johnson said: “It is time that we got our confidence back. We don’t need laws to compel people to be considerate to others. We will encourage people with Covid-19 symptoms to exercise personal responsibility, just as we encourage people who may have flu to be considerate to others.”
27th Feb – Mail on Sunday newspaper: The Unvarnished Truth by Lord Ashcroft & Isabel Oakeshott
Last summer, the NHS was awarded the George Cross by the Queen. In a hand-written personal message, she said: “Over more than seven decades, and especially in recent times, you have supported the people of our country with courage, compassion and dedication, demonstrating the highest standards of public service”.
Most people would agree with this sentiment, particularly in light of the heroic response of the frontline workers to the coronavirus pandemic. Curiously, in a development that says much about Britain’s relationship with its favourite institution, the perception that we had a deteriorating health service appeared to be turned on its head during the pandemic itself. The bleaker things got, the greater the people’s adulation. The NHS is often compared to a national religion. Even without a global health crisis, it perennially tops voters’ concerns, which makes the debate over how it is run and funded extremely sensitive. Sadly, politicians and many of those who run the NHS wilfully deceive the public about the quality of service they receive. The aim of our new book is to strip away such spin and paint a picture of the NHS as it really is: the good, the bad and the ugly. It is only by knowing the truth that the country can demand better.
Extensive research among focus groups at the outset of the pandemic in March 2020, and again last November when the crisis eased, showed that people were impressed by the way the service had responded to an unprecedented situation. Nonetheless, most (rightly) believed the NHS is in a worse state than it was before the crisis began. To provide some depth, we carried out a special investigation into the state of the health services in one particular part of the country. Prompted by disturbing evidence about standards of care, we selected the Isle of Wight. Until very recently, the island was one of the worst-performing NHS Trusts in England and a dangerous place to be seriously sick. An assessment by the Care Quality Commission (CQC), who are the Independent Regulator of Health and Social Care Services in the UK, in 2017 concluded that the trust was failing on multiple levels and was guilty of an array of safety breaches. Inspectors ruled that there were insufficient staff; medical care was inadequate; end-of-life care was ‘dire.’ During official investigations into 35 unexpected deaths in 2018/19, several themes cropped up with depressing regularity. They included overcrowding; breaching A&E waiting-time targets; doctor shortages; use of agency nurses; poor staff communication; poor medical record-keeping; inexperienced doctors; clinical staff shortages; and inadequate IT systems. More sinister in May 2019, the trust admitted to ‘failing terribly’ in not disclosing abnormalities over the deaths of patients. The island’s coroner, Caroline Sumeray, said the trust failed to inform her of 20 serious incident investigations before the bodies were cremated, meaning the truth about how patients died, and the hospital’s role in their demise, could not be uncovered at St. Mary’s Hospital in Newport.
Unfortunately, former health secretary Matt Hancock’s efforts to digitise the entire NHS were somewhat derailed by the coronavirus – though the pandemic showed how fast and effectively the machine can move in an emergency. The NHS app was rapidly improved and (for better or worse) online consultations became mainstream. Nonetheless, parts of the NHS remain in the digital dark age, particularly when it comes to patient records. Huge sums, right across the NHS, are squandered procuring software that are unfit for purpose and must then be upgraded, repaired or changed, usually by the same company that failed to provide what was required in the first place.
During his time at St. George’s Hospital in Tooting, South-West London, Mark Gordon, who spent years working as an interim chief operating officer within the NHS, recounting the introduction of a system known as ‘Cerner’, he recalls that it descended into chaos because people did not understand how it worked. Gordon claims that as many as two million patient records were lost during the fiasco in 2017. He continues: “We started to find 300 patients a week who were potentially harmed, and that was only out of a sample of 650,000 of two million lost records.”
Professor Sir Brain Jarman OBE is an 88 year-old academic who probably knows more about hospital mortality than anyone else in the world. Now an emeritus professor at the School of Public Health, Facility of Medicine at Imperial College London, he is best known for developing a way of measuring whether hospitals have higher or lower death rates than expected. Jarman’s methodology adjusts patient data for factors such as age, gender, deprivation levels and whether patients were admitted as an emergency. The aim is to create a reasonable measure of the quality of care. With depressing predictability, managers soon figured out that if they gave more patients a ‘palliative care’ code – meaning those patients were assumed to have come to hospital to die, and thus the hospital could not be criticised for failing to save them – they could dramatically reduce official death rates. In another fiddle, hospitals found that they could reduce death rates by discharging dying patients to hospices.
Well done for staying with that last article good reader! Well worth the effort I’m sure you’ll agree. With the continued figures indicating that slowly but surely in the Western World, we’re coming out of this pandemic, as flagged in this month’s Health News, with many businesses finally beginning to gain some more material traction, with many employees being back at the office to some extent, with folk actually planning their summer holidays, abroad, of all places, (without having to fill out that dreaded passenger locator form, and without the need for multiple costly testing) hope is in the Spring health air, if not ‘global peace air’.
Until April please continue to be mindful of the outgoing air-borne killer called COVID-19, and enjoy the blossoming daffodils, snowdrops and burgeoning chirpier birdsong!
Warmest regards,
Daniel Donoghue,
Brokerage Director
Surrey Circle Health



{kind=link}
{kind=link}
{kind=link}